
Bias and prejudice against practitioners is more common than you might think. Many documented case studies show how terrible and insensitive patients have been to those who are trying to help them most. Here are a couple examples:
- A black physician, Tamika Cross, attempted to help a sick passenger on a flight and is told by a flight attendant they needed “actual physicians or nurses.” Leon McDougle, a black resident was informed by the husband of a woman in labor that a man of his race would not be taking care of his wife (out of a dozen interns, McDougle was the most educated in obstetrics). Dorothy Novick took over for her colleague from Colombia after a six-year-old patient says, “I don’t want some spic doctor, I want the other lady!” The father agreed.
- Lachelle Dawn Weeks describes a time when she helped an elderly patient who complimented her on making it to medical school, but advised, “Now, don’t waste your affirmative action.”[iii] Weeks had become aware of bias in even stronger form with colleagues. A female Muslim doctor was given a long explanation of how all Muslims are terrorists and ruining the world—the patient was an elderly veteran. A Vietnamese colleague told her she was once called a “dirty incompetent g**k” by an alcohol withdrawing patient.
- Seema Yasmin saw a patient that assumed she is not a doctor, and upon learning she was, replied, “I don’t like your kind, I want a white doctor. A man.” Yasmin is Indian and female. Her reply was simply, “OK”, and as she left the room, her cheeks burned. This was not the first time she had experienced sexism and racism from patients. Sure, they were not all blatantly racist requests for male and/or white doctors, but “sly digs at my competence on the basis of my name, the color of my skin or my dresses.” “You’re too pretty to be a doctor.” “Get me someone who went to medical school, not beauty school.” Yasmin writes that after running around the hospital to find a white male doctor (ultimately a non-white male had to suffice), she was called away to an emergency case, “shoving my shame and relief into blue latex gloves, and never mentioning again what had happened.”
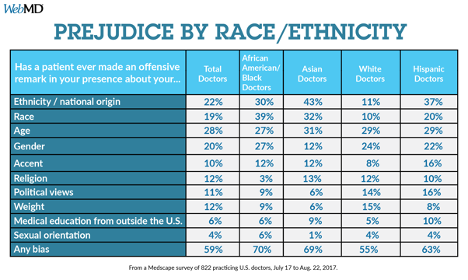
If you are one of 59% of doctors saying they’ve experienced bias from their patients according to a 2017 Medscape survey, you may have an intimate understanding of the emotional impact it can have.
One of the questions in the Medscape survey was, “Has a patient ever made an offensive remark in your presence about your Age, Gender, Ethnicity, Race, Weight, Sexual Orientation, Religion, Accent, Political Views or Medical Education outside the US?”
As you can see from the table below, the odds of being the subject of prejudice at least at some point in your career is fairly high.
Singh et al notes more subtle racism may manifest in less cooperation with history taking and examination, or other behaviors that may not be immediately noticed.
What may appear to be bigotry, may indeed be something else. For example:
- A patient would simply feel more comfortable with a provider of the same sex or race. This could be a result of religious mandate.
- A patient has a history of discrimination, trauma or mistrust on an individual level or as a member of their racial/cultural group.
- A patient is simply having a hard time understanding the provider due to accent or language differences.
- A veteran patient is suffering PTSD and a provider reminds them of former enemy soldiers. Or any post-trauma of any origin that is triggered by the provider.
While situations like these may initially present misplaced fears or anger seeming to be bigotry it is important for you to understand there may be underlying factors causing their concerns. While doing the right thing to help with those concerns may be best for the patient it is also important to know that, as a highly trained professional, abuse and aggressive behavior should not be tolerated. The American Medical Association Code of Ethics states one may, “Terminate the patient-physician relationship with a patient who uses derogatory language or acts in a prejudicial manner only if the patient will not modify the conduct. In such cases, the physician should arrange to transfer the patient’s care.”
We Can Help
The topic of bias towards physicians by patients has gained more attention recently, and there is no doubt more to come regarding research, management of these behaviors, ethical and legal implications. If you are troubled by this topic, or have experienced or witnessed these types of biases, you should share this with your leader. Additionally, you can reach out to VITAL WorkLife to talk with a peer coach about this issue.
Physician Well Being Resources members can access their resources, including peer coaching, by calling 877.731.3949 or through the VITAL WorkLife App.
For more information:
- Several articles on patient bias from Medscape. https://www.medscape.com/sites/public/patientprejudice2017
- One-hour presentation by Kimani Paul-Emile, J.D., Ph. D⁷. Dealing with Racist Patients: Guidance for Trainees and Educators. https://www.youtube.com/watch?v=HAEVXaAJxhk
Sources:
Singh K., Sivasubramaniam, P., Ghuman S., & Mir H. The dilemma of the racist patient. The American Journal of Orthopedics. 2015 Dec;44(12): E477-9.
Weeks LD. When the patient is racist, how should the doctor respond? STAT. https://www.statnews.com/2017/06/12/racism-bias-patients-doctors/. Published June 12, 2017.
Watson S. Credentials don't shield doctors, nurses from bias. WebMD. https://www.webmd.com/a-to-z-guides/news/20171018/survey-patient-bias-toward-doctors-nurses?ecd=medscape. Published October 18, 2017.
Novick DR. Opinion: racist patients often leave doctors at a loss. The Washington Post. https://www.washingtonpost.com/opinions/racist-patients-often-leave-doctors-at-a-loss/2017/10/19/9e9a2c46-9d55-11e7-9c8d-cf053ff30921_story.html?utm_term=.d6ef367d93d1. Published October 19, 2017.
Yasmin S. Patients Discriminate Against Doctors: A Muslim Physician Weighs In. https://www.medscape.com/viewarticle/878408. Published April 14, 2017.

